 Listen Now:
Listen Now: February 01, 2022
Dr Rawiri Taonui: Urgent need for Māori Omicron strategy

A Māori Omicron Strategy
With 398 new community cases over the last four days, Omicron has truly entered the whare of Aotearoa. The immediate priority right now is a Māori Omicron Strategy. Eight weeks after the first Omicron case arrived in New Zealand, there is no Māori plan.
Late last year, the Government’s Māori caucus led an effective $120 million two tranche rollout supporting Māori vaccination and community-led protection. Māori cases fell an average of 26.9 per cent per week during five weeks over Christmas compared to 19.8 per cent for non-Māori.
While the decline was impressive, the Government framed those initiatives in a Delta environment. Omicron presents a next-level hyper-transmissible risk.
Experience in countries where Omicron arrived earlier than in Aotearoa shows the variant is exploiting lower indigenous vaccination rates, poorer health profiles, socio-economic deprivation, over-crowded housing and lack of access or distance from health services.
Canada has had 6,851 Omicron cases in First Nations communities since late November. This is despite First Nations having higher 12-years+ full vaccinations than Māori (86 per cent to 78.5 per cent) and 5-to-11 years vaccinations (43 per cent to 15 per cent).
On 20 January, Indigenous Health Services Canada responded with a $125 million ($NZ149.6 million) package to update, review and activate Omicron response plans, provide resources to reinforce child vaccinations, 12 years+ vaccination and boosters, supply bulk rapid antigen tests, and increase surge capacity in community infrastructure and staffing to cover higher infections and staff gaps through sickness, and to provide food security and resources for home-isolation.
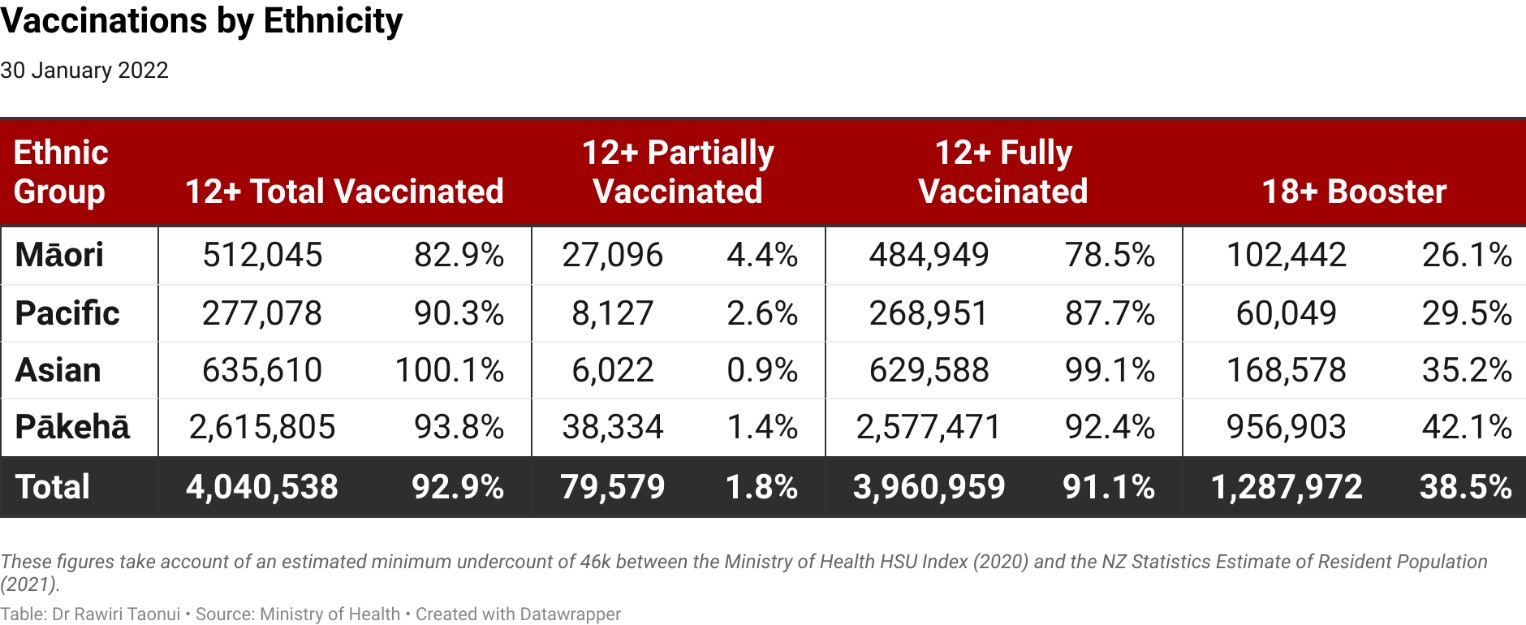
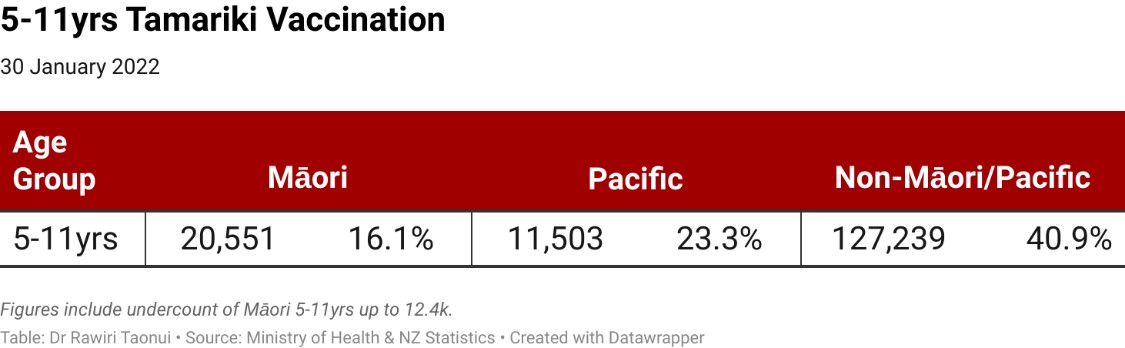
Māori require a similar strategy focussed on vaccination and home isolation lest Omicron overruns our communities. Māori are exposed. On Sunday we were 10.0 per cent behind the national figure for total vaccinations, 12.6 per cent behind on full vaccination, 12.4 per cent behind on boosters, and 23.4 per cent behind in the tamariki vaccination rollout.
Support for Home Isolation
Omicron will see large numbers of Māori isolating at home. Families will need a reserve of food lasting at least a few days. Basic medical supplies like paracetamol, ibuprofen, cough syrups, fluids and vapour rubs will mitigate symptoms. Higher-quality masks or double-masking are important against an airborne efficient Omicron. Disinfectants for surface cleaning are also vital. Most Māori will isolate in homes with one toilet which will require cleaning after every use.
Many whānau Māori will be unable to afford these items. Those in remote areas will face difficulties accessing supermarkets and shops. Having a whānau contact person deliver food as recommended by the Ministry and government, will be difficult if not impossible if Omicron impacts whole communities particularly in rural-urban or remote areas. Ordering food deliveries in remote areas is often not possible and supply chain disruptions a real eventuality.
Recommendations supporting Māori home isolation:
- Resourcing to help whānau and communities to prepare home isolation plans, including how to care for the sick and protect the uninfected, and where to get help.
- ‘Kāinga Packs’ including a food parcel, basic medicines, basic medical supplies like decent quality masks, cleaning supplies and disinfectants.
- Support for more staffing in marae, hapū and community organisations to cope with higher case numbers and cover staffing gaps through sickness.
- Strengthen sick leave provisions for workers and paid sick leave for caregivers to enable whānau to stay home when unwell or look after others.
Strengthen Māori Vaccination
Continuing lower vaccination rates place Māori at significant risk. There is a need for more direct communication and consultation with Māori on the flagging booster and tamariki rollouts through the appointment of a Māori Vaccination Monitoring Group. This should have full access to data, Ministry officials and the Māori members of Cabinet. The Government should also reinforce the Māori health provider and community vaccination workforce which will face increasing pressure in the face of Omicron.
Reduce Booster Wait to Three Months
Current evidence is that a single dose of the Pfizer vaccine is weaker against Omicron and the efficacy of double vaccination gradually wanes. The evidence also shows that a third booster shot provides increased protection.
As above, Māori are 12.4 per cent behind in booster vaccinations. Much of this is attributable to last year’s age-centred vaccination which pushed Māoridom’s more youthful population to the end of the queue.
Māori health providers have led a magnificent effort closing a mid-September 25.2 per cent gap between total Māori vaccinations and the national rate to 10 per cent. An unintended consequence of the catch-up is that more than 108,000 Māori vaccinated since 1 November will not become eligible for a booster shot until 1 March. That is too late. Moreover, a considerable number of the 27,000 partially vaccinated Māori (the highest proportion of all ethnicities) sitting on first vaccinations will qualify even later.
The Government must bridge this inequity by shortening the time to receive booster shots to three months. Britain, South Korea, Thailand, France and Germany have adopted the three-month standard. Last week, in response to record cases, New South Wales and Victoria reduced the wait for booster shots to three months.
Lifting Tamariki Māori Vaccination
Indigenous children face additional risks with Covid-19 because of their living situations, health inequities and racism. By August last year, Aboriginal children made up 40 per cent of Covid-19 cases in western New South Wales. By mid-January this year, tamariki Māori were 53 per cent of all cases and 63 per cent of all hospitalisations under-12 years in Aotearoa.
Ministry of Health vaccination data says 18.0 per cent of tamariki Māori are vaccinated compared to 33.0 per cent for all ethnicities. The gap is much wider.
Firstly, the Ministry does not compare Māori with non-Māori, which lowers the higher national figure closer to that for Māori.
More concerningly, the Health Service User (2020), which the Ministry uses to calculate the number of vaccinations, counts 115,562 tamariki. This is well short of 127,980 tamariki in the NZ Statistics Estimate of the Resident Population (2021) meaning there is an undercount potentially over 12,400. A more accurate calculation of the tamariki vaccination is 16.1 per cent for Māori compared to 40.9 per cent for non-Māori/Pacific.
The Government must prioritise the tamariki vaccination rollout to avoid repeating further inequities in the first vaccination rollout. This includes targeting low decile schools with large Māori enrolments when they re-open this week.
Last year’s vaccination rollout failed because it did not allow Māori to vaccinate as whānau. The tamariki rollout can avoid the same mistake by ensuring all whānau members are vaccinated. Encouraging combined adult booster and tamariki vaccination is a useful way forward.
The current wait time between two doses for tamariki is eight weeks. The Government should consider the advice of the US Centres for Disease Control and Prevention (CDC) and reduce this to three weeks to close the gap between Māori and national child vaccinations.
Release Tamariki Māori Vaccination Data
The Ministry of Health must immediately release tamariki Māori data to the Whānau Ora Commissioning Agency and other Māori health providers. The Director-General of Health Dr Ashley Bloomfield has said he needs to consult about privacy before releasing this information.
There are two main health databases. The National Health Index (NHI) contains the name and ethnicity of persons using the health system but not their vaccination status. The COVID Immunisation Register (CIR) contains the name and vaccination status of individuals but not their ethnicity.
Whānau Ora have access to the NHI system but not the CIR. Other providers like Healthline have access to the CIR. Last year, the High Court found that there was no concern of Whānau Ora breaching the privacy of individuals. Withholding Māori vaccination information from Māori providers is therefore discriminatory.
Last year, Dr Bloomfield said he withheld data in some areas because some iwi disagree with releasing their data. The perverse anomaly here is that neither the NHI nor CIR contains any iwi data. If an iwi in one region objects to the release of data, there is no way of separately identifying their tribal members living in other areas and withhold their information. Conversely, it is impossible to identify Māori within their region whose iwi outside the region agree with releasing their data.
Playing iwi and Whānau Ora off against each other is inconsistent with te tiriti. It is not the kāwanatanga role of the Pākehā to arbitrate between Māori groups or the rangatiratanga role of Māori to mediate between mainstream government ministries.
The Ministry’s position also contradicts the spirit, content and directives of two High Court decisions from Justice Cheryl Gwyn on Māori data in early and late November last year. One of Justice Gwyn’s pertinent observations was that it is inconsistent for the Ministry to impose a different standard of privacy on Māori health providers regarding Māori data but not on mainstream providers.
The Ministry’s position also contradicts Iwi Chairs Forum Pandemic Response Group co-chair Mike Smith who has said the Ministry should urgently give the Whānau Ora Commissioning Agency access to vaccination data for tamariki Māori. Last year, the Minister of Health Andrew Little and Minister of Māori Development Willie Jackson also supported the release of the data.
A prevailing narrative makes much of Māori mistrust of the Government. We should have greater concern about the Ministry’s obstinate mistrust of Māori. Playing iwi off against Whānau Ora only sabotages the tamariki Māori vaccination effort.
Strengthening Māori vaccination recommendations:
- Appoint a Māori Vaccination Monitoring Group broadly representative of Māori with access to key data and able to speak directly with the senior officials in the Ministry of Health and Māori members of Cabinet.
- Reduce the wait time for booster shots from four to three months.
- Resource and strengthen the Māori vaccination effort including the recruitment and training of more vaccinators.
- Provide bulk rapid antigen tests (RAT) to Māori health providers and community organisations.
- Prioritise the 5-to-11 years tamariki Māori vaccination rollout.
- This includes a specific focus on vaccinating in low decile schools with large Māori enrolments when they open this coming week. This should include ensuring other whānau members living with tamariki are vaccinated.
- Reduce the eight week wait time between 5-to-11 years vaccinations from eight weeks to three.
- The Ministry of Health must immediately release tamariki Māori vaccination data to Māori health providers.
Daily Māori cases are currently quite low. These numbers will begin growing once schools start back. There is an urgent need for a Māori Omicron Strategy.
Noho haumaru, stay safe.
Dr Rawiri Taonui







