Listen Now:
Listen Now: April 16, 2020
Dr Rawiri Taonui | Cultural Decoding Under-Testing for Māori and Pacific Peoples

Cultural Decoding Under-Testing for Māori and Pacific Peoples
Dr Rawiri Taonui
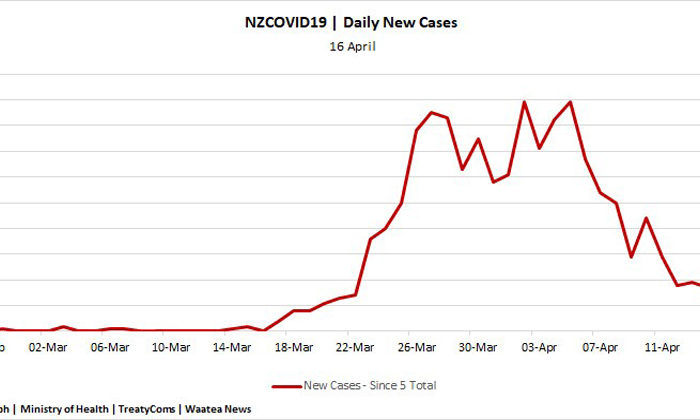
Data from COVID-19 testing in late March and early April confirms the concerns of many Māori and Pacific Peoples health leaders and community workers about under-testing in our communities. This includes during the first phase of testing focussed on New Zealanders who had travelled overseas, and the early part of the new criteria applied on 1 April including to target Māori and Pacific communities.

Engagement and Bias
Community leaders and workers are saying mainstream testing sites do not engage well with Māori and Pacific Peoples, and, based on previous experiences of health care, many Māori and Pacific engage better with sites staffed with our people.
Others believe more Māori and Pacific have been declined tests. There is not enough data available to substantiate this claim, although the writer has seen data from one testing site over one week, which shows 50% of Pacific and 16% of Māori were declined tests.
This could be related to the early and necessary emphasis on testing travellers. In other circumstances, this is no excuse. For example, in the Marist Girls College cluster, Geoff Muliaga Brown and a member of another family, both linked to a fiafia night where there was secondary transmission, were each twice denied tests on the basis they had not travelled overseas despite experiencing obvious and serious COVID-19 like respiratory symptoms.
Māori health operators also believe systemic bias is playing out in the COVID-19 response. They believe some District Health Boards (DHBs) view Māori testing sites unnecessary or less competent. This seems to vary. DHBs with Māori and/or Pacific managers have more confidence in Māori and Pacific health providers. Those who do not tend to be more dismissive.
One operator said, that for this reason, they found Counties-Manukau better to deal with than Canterbury. Their anecdotal observation finds support in the report Whakapuāwaitia Ngāi Māori – Thriving as Māori 2030 (2012), which although dated, says Māori are 8% of corporate and 14% of support and care staff in the Counties-Manukau DHB but only 1% of corporate and 5% of support and care in the Canterbury DHB.
Another manager of a licensed Māori General Practice used the phrase ‘set up to fail’. Their DHB reportedly agreed to use their premises for testing, declined to use the practice’s staff, brought in other DHB staff then proposed closing because less than 100 tests were processed during the first week. The point is the practice staff could have conducted tests and then undertaken other duties when testing was slow.

Information
Health officials have not been forthcoming with enough data to confirm or assuage these concerns. After several official information requests, the Ministry did release national figures of 40,000 tests to April 9, including by ethnicity but unhelpfully not by DHB. The Nelson-Marlborough (NMDHB) and Northland DHBs (NDHB) have separately provided this writer with useful one-week snapshots and by ethnicity. I also have informal releases of information.
Other DHBs are reluctant to release data. The Auckland DHB has a policy of not processing requests for information until after the COVID-19 emergency. The Waikato DHB is publishing testing information online but does not include data for Māori and Pacific. Of other DHBs, seven referred the request to the Ministry, one referred to an internet page that had no information, several did not respond.
National Data
The national data shows that to 9 April, Pākehā and Others at 66.3% of all tests were tested above their demographic of 64.2% on the Ministry of Health model of population. Their rate of 8.6 tests per1000 persons was also above the average of 8.1. Asians and Māori were below both their demographic and the average tests per1000.

Pacific were above demographic on both measures. That figure is possibly influenced by testing of Pacific students and their families (about 180 students) associated with the Marist College cluster. 300 individual Pacific tests in that cluster would push the national figure for Pacific below demographic and the 8.1 average for tests per1000.
This interpretation of the Pacific data finds support in an informal release from the Waitematā DHB. Chief executive and Northern Region COVID-19 lead, Dr Dale Bramley, is quoted saying that 17,000 tests in ‘Auckland’ since 21 March included 20% Māori or Pacific. The latest 2020 population estimate for wider Auckland says the combined Māori/Pacific population is 25.3%. In Counties-Manukau, 36%. Testing is below demographic.
The national data also covers a period extending 8 days after the assessment criteria were changed, including to prioritise Māori and Pacific. The differential levels already noted, therefore, support a conclusion that Pākehā were over-tested and non-European Māori, Pacific and Asians under-tested during both the first phase focused on travellers and during the early part of the second phase supposedly prioritising Māori and Pacific.

Nelson-Marlborough DHB
Data available from two regional DHBs further supports this conclusion. Data from the NMDHB to 5 April also shows that Pākehā were tested above demographic and tests per1000, and, Māori and Pacific below demographic and tests per1000.

Northland DHB
Data from the NDHB to 1 April, also shows that Pākehā were tested above demographic and per1000 and Pacific below on both. The Māori figure is on par. A key factor in this better outcome for Māori, again from Whakapuāwaitia Ngāi Māori, shows the Northland DHB has the third-highest percentage of Māori DHB corporate staff (16%) and DHB support and care staff (28%) of all DHBs, and many more than the lower ethnic testing Nelson-Marlborough DHB with the fifth-lowest number of Māori at corporate (5%) and fourth lowest in support and care (6%).

Information as Privilege
To identify areas and regions that need to be targeted with more testing, we need the data on testing by ethnicity from each DHB. Information is not privilege. In a crisis, information is a human right. Withholding that information constitutes white privilege risk management of Māori and Pacific community data. Information is power and our communities require this information to empower them in their fight to defend their papakāinga and aiga. There is a massive nation-wide effort from our communities that has thus far prevented our becoming, yet again, the primary victims of another epidemic. It is all action, in multiple places and in all directions at once. Having this data will inform where Māori and Pacific need to focus their energy. Testing must be more thorough in our communities to uncover any yet undetected residual reservoirs or clusters.
The Paradox of a Pākehā Pandemic
If there is a paradox here, then it is that so far in New Zealand, this is mainly a Pākehā epidemic. COVID-19 has spread internationally because of unprecedented borderless travel. More Pākehā appear to have travelled and consequently, more have been infected. More have spread COVID-19. Based on the 15 April Ministry of Health live daily briefing, 74.2% of total cases are European and others, nearly 10% more than their demographic on the Ministry model of population.
In a further paradox, the Māori and Pacific cultural practice of looking after our elders at home seems to have added a layer of protection. With COVID-19 threatening several aged care facilities, the older age to which Europeans live and that they comprise over 90% of the patients and residents in aged care facilities, combines to make them currently the most vulnerable section of the populace. They comprise all deaths to 15 April.
Suffering is not a cross-cultural race. As Māori and Pacific, we need to support as much testing in this group as is required for their care and protection. However, what is unfolding in aged care facilities portends what could unfold in our communities if we do not properly test Māori and Pacific. Historically, we have lost more lives in epidemics than the Pākehā population, acquire at a younger age the comorbidities that COVID-19 so ruthlessly exploits, have experienced racism and differential assistance in previous epidemics and continue to experience that in contemporary health care.
Māori and Pacific must be tested above-demographic. We can also note that as of today, New Zealand is testing at the rate of 14,000 tests per million of population. That figure, not total tests, constitutes the key index to the effective discovery and control of COVID-19. In no small way, our situation is assisted by the fact that we have more recovered (770) than active cases (631), another key index of control over the virus. A way forward, to address both pockets of infection and ensure we properly test Māori and Pacific, is to maintain Level 4 or a controlled Level 3 and lift testing per million by triple. Countries, such as Norway and Switzerland are well past 20,000 tests per million and others over 30,000 tests per million.
Test
On 1 April, the Ministry announced a broadened criterion for testing and this last Monday, said it would focus on the regions and Māori communities. Healthline now asks if you are Māori or Pacific. There are now 70 CBACs, including many with mobile capacity. There are 14 CBACs in Auckland. There are more Māori and Pacific operated sites. They are doing tremendous work. Whānau Ora Community Clinic in Wiri and South Seas Healthcare in Ōtara reports that more than half the people tested at these sites have been Māori or Pacific.
Noho haumaru, stay home, stay safe, stay self-sovereign, test the people.
 &
& 
Copyright © 2020, UMA Broadcasting Ltd: www.waateanews.com